|
TELEPATHOLOGY |
|
|
Is the practice of pathology at a distance. It is the acquisition of histological, cytological and macroscopic images for transmission along telecommunication pathways for diagnosis, consultation or continuing medical education.1 It involves essentially, viewing images on a video monitor and rendering a diagnosis. |
|
|
APPLICATIONS OF TELEPATHOLOGY |
|
|
It is especially useful for a solo pathologist practicing in a remote area, who requires an immediate second opinion, for a case where subsequent management decisions would be based on his report. It can be especially useful in for frozen section consultations1. In addition, it can be used as a tool for quality assurance, teleconferencing and continuing medical education programmes2. Higher centres, which find it difficult to attend to increasingly larger numbers of patients, can use this as a tool to render their services more patients. |
|
|
TELEPATHOLOGY SYSTEMS |
|
|
A telepathology system is comprised by: |
|
|
|
|
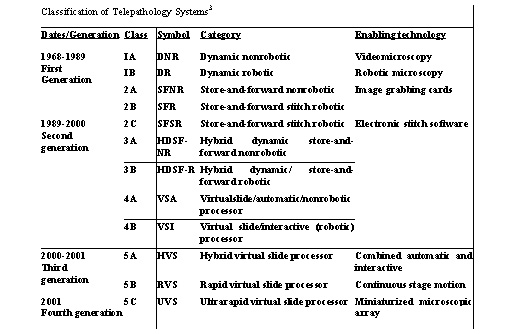
The table shows various generations of telepathology systems.3 DYNAMIC TELEPATHOLOGY (Real Time Telepathology)1,4,5 |
|
|
Is a telecommunication procedure for viewing live images or a sequence of images at real time. It includes remote operation of a microscope and examination of slides from a distance. The system has three requirements: |
|
|
|
|
Advantages |
|
|
|
|
Limitations |
|
|
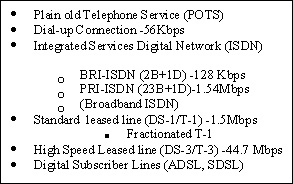
The major limitations are the cost and the necessity of a high bandwidth, to the tune of 1.54 Mb/s for transmission. |
|
|
STORE AND FORWARD TELEPATHOLOGY (static telepathology)4 |
|
|
Is the practice of pathology at a distance, based on transmission through telecommunication means of still or stationary images from pathology specimens for their corresponding interpretation and diagnosis. It requires necessarily that the referring person is a competent professional pathologist with basic knowledge in pathology informatics. At the receiving centre also there is a pathologist who receives the electronic images and performs the interpretation and diagnosis. |
|
|
Advantages |
|
|
|
|
Limitations1,4 |
|
- Inability of the Consultant to scan the slide at low power - inability to identify significant areas at low power. - Referring pathologists tend to select images which support their own diagnosis. - Limited number of images may under-represent the complexity of the case.
|
|
|
|
|
|
Accuracy of Diagnosis 1,6,7 |
|
|
Accuracy rates of 77% to 99% have been reported by various authors. The studies however, are not comparable, because different methodologies have been employed and the number of participating pathologists in each study is also variable. However, notably, the Arizona International Telemedicine Network has reported a concordance (between the Telepathology diagnosis and glass slide diagnosis) rate of 88.5% and they found a 96.5% concordance for clinically important diagnoses. Weinstein et al have reported a concordance rate of 99%. |
|
|
HYBRID DYNAMIC STORE AND FORWARD SYSTEMS4 |
|
|
These systems are based on a combination of dynamic and static systems and are more cost-effective. |
|
|
STATIC TELEPATHOLOGY |
|
|
Static Telepathology being more relevant in the Indian context, because of lower cost of equipment and telecommunication costs and the lack of broadband linkages4, will be discussed in more detail. The workstation of a static telepathology system is comprised by : |
|
|
|
|
Image Acquisition8 |
|
|
Any of the following methods of image capture may be used : |
|
|
|
|
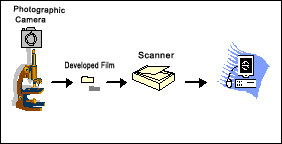
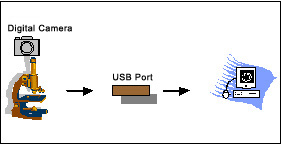
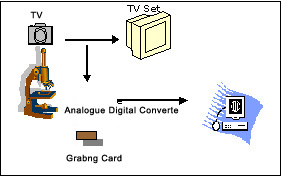
One can use conventional photography using a camera mounted on a microscope, and have the film developed and take prints of images, if that is the only method of image capture available and one does not want to invest further. In this case of course, one would end up spending extra time in having the film developed. One could also use analogue cameras or television cameras to capture images which have been used in the past for display purposes. As of today, however, digital cameras are being used increasingly since they are easy and more convenient to use and are available at increasingly economical prices. Both analogue and digital cameras capture images in the wave form (analogue images) using charged couple devices (CCDs), commonly known as microchips. |
|
|
The important thing is that images have to be in the digital format in order to permit transfer to a computer, which is necessary to permit transmission of images using internet. While photographic images can be digitized using a scanner, images obtained from an analogue camera are converted into the digital format using analogue to digital converters (ADCs), digital cameras have inbuilt ADCs and therefore, give digital images immediately. |
|
 |
 |
 |
|
|
Digital Camera 1,8 |
|
|
Digital cameras available these day are either single-chip cameras or three chip cameras, meaning thereby that they have either a single microchip or three chips inside. A single chip camera offers one third the luminance resolution, because the same CCD accommodates the three primary colours in alteration, whereas a three chip camera has three identical CCDs (each handling a single primary colour) and offers full resolution of an image, which is closest to the true image, this however, is almost triple the cost and there is also a proportionate increase in file size (as explained below). |
|
|
It is recommended that a single chip camera with a resolution of 3 to 5 megapixels gives optimum images for routine static telepathology purposes. |
|
|
Digital Imaging 1,8 |
|
|
Digital images are either vector images or raster images. For Telepathology purposes, raster images (bitmaps) are use and will therefore, be discussed. |
|
|
|
|
|
|
Colours and Resolution |
|
- 2 (21) colours in a pixel
- 256 (28) colours in a pixel (1 byte)
- 16.8 (224 ) million colours in a pixel (3 bytes, one each for a primary colour). |
|
|
|
|
Resolution is in direct relationship with the amount of pixels per unit of longitude - the larger the no. of pixels captured per image, the higher the resolution. |
|
|
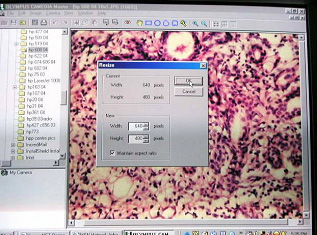
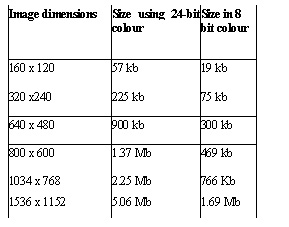
= number of dots per inch (dpi) or pixels per inch (ppi). File Size = width in pixels x height in pixels x bit depth in bits eg : 640 x 480 x 8 = 2457600bits/8 (1byte=8bits) = 307200 bytes = 300Kb (1kb=1024 bytes) Recommended Size for transmission
|
 |
|
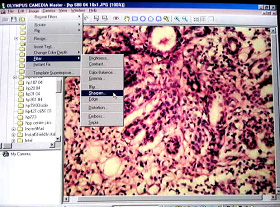
Image Compression |
|
|
Since large sized images come in the way of easy transmission, it is recommended that images of = 1 Megapixel (1MB) should be compressed. Image compression could be |
|